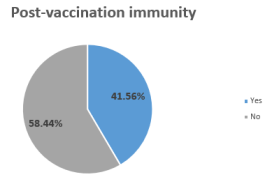
Introduction: Vaccination remains the primary strategy against COVID-19. However, data may not reflect actual population immunity. This study aims to determine the seroprevalence of post-vaccination immunity against COVID-19 in Benin and identify associated factors. Methods: A cross- sectional descriptive and analytical study was conducted from April to September 2023 in 21 hospital centers across Benin's twelve departments and included 3802. Post-vaccination immunity was defined by the presence of anti-SARS-CoV-2 Spike IgG antibodies and the absence of anti-NCP IgG antibodies, using the Euroimmun ELISA test. Data were analyzed using STATA software with multivariate logistics regression. Results: Seroprevalence of post-vaccination immunity was 41.56%. In multivariate analysis, factors associated with this immunity were age (adjusted OR=1.56; 95% CI [1.09-2.59]), residence within the former sanitary cordon (aOR=1.34; 95% CI [1.14-3.01]), history of hypertension/cardiovascular disease (aOR=3.25; 95% CI [1.41-4.63]), and history of diabetes (aOR=2.73; 95% CI [1.89-3.93]). Conclusion: Post-vaccination immunity is higher among vulnerable groups (elderly, comorbidities) and those in strategic urban zones, reflecting the prioritization of vaccination campaigns. Recommendations are proposed to target younger populations and rural areas to strengthen collective immunity.
| Published in | World Journal of Public Health (Volume 11, Issue 1) |
| DOI | 10.11648/j.wjph.20261101.12 |
| Page(s) | 11-19 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
COVID-19, Post-vaccination Immunity, Age Comorbidities, Benin
Variables | Post-Vaccination Immunity, Yes (n=1580) | Post-Vaccination Immunity, No (n=2222) | p-value |
|---|---|---|---|
Sex | 0.31 | ||
Male | 698 (44.2%) | 1003 (45.1%) | |
Female | 882 (55.8%) | 1219 (54.9%) | |
Age (years) | < 0.001 | ||
Mean (SD) | 38.2 ± 15.1 | 32.5 ± 16.9 | |
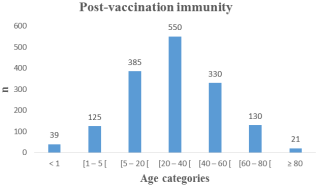
Age Group (years) | 0.002 | ||
< 1 | 39 (2.5%) | 60 (2.7%) | |
1 – 4 | 125 (7.9%) | 179 (8.1%) | |
5 – 19 | 385 (24.4%) | 596 (26.8%) | |
20 – 39 | 550 (34.8%) | 762 (34.3%) | |
40 – 59 | 330 (20.9%) | 419 (18.9%) | |
60 – 79 | 130 (8.2%) | 174 (7.8%) | |
≥ 80 | 21 (1.3%) | 32 (1.4%) | |
Living environment | 0.08 | ||
Urban | 608 (38.5%) | 913 (41.1%) | |
Semi-rural | 456 (28.9%) | 685 (30.8%) | |
Rural | 516 (32.7%) | 624 (28.1%) | |
Residence within sanitary cordon | 0.002 | ||
Yes | 380 (24.1%) | 380 (17.1%) | |
No | 1200 (75.9%) | 1842 (82.9%) | |
Monthly income (CFA Francs XOF) | 0.65 | ||
Refusal to answer | 61 (3.9%) | 87 (3.9%) | |
< 50,000 | 458 (29.0%) | 645 (29.0%) | |
50,000 – 150,000 | 616 (39.0%) | 867 (39.0%) | |
150,000 – 250,000 | 316 (20.0%) | 444 (20.0%) | |
> 250,000 | 129 (8.2%) | 179 (8.1%) | |
Socioeconomic level | 0.51 | ||
Very low | 237 (15.0%) | 333 (15.0%) | |
Low | 474 (30.0%) | 667 (30.0%) | |
Average | 553 (35.0%) | 778 (35.0%) | |
High | 237 (15.0%) | 333 (15.0%) | |
Very high | 79 (5.0%) | 111 (5.0%) | |
Education level | 0.15 | ||
Not enrolled | 506 (32.0%) | 711 (32.0%) | |
Primary | 442 (28.0%) | 623 (28.0%) | |
Secondary | 395 (25.0%) | 556 (25.0%) | |
Higher | 237 (15.0%) | 333 (15.0%) | |
Occupation | 0.41 | ||
Unemployed | 316 (20.0%) | 444 (20.0%) | |
Student | 237 (15.0%) | 333 (15.0%) | |
Factory worker | 253 (16.0%) | 355 (16.0%) | |
Merchant | 380 (24.1%) | 532 (23.9%) | |
Civil Servant / Manager | 394 (24.9%) | 558 (25.1%) | |
Ethnic group | 0.78 | ||
Dendi | 300 (19.0%) | 422 (19.0%) | |
Bariba | 300 (19.0%) | 422 (19.0%) | |
Fon | 442 (28.0%) | 623 (28.0%) | |
Goun | 332 (21.0%) | 466 (21.0%) | |
Other | 206 (13.0%) | 289 (13.0%) | |
Household size | 0.91 | ||
≥ 5 | 1027 (65.0%) | 1444 (65.0%) | |
< 5 | 553 (35.0%) | 778 (35.0%) | |
Religion | 0.35 | ||
Christian | 695 (44.0%) | 978 (44.0%) | |
Traditional | 111 (7.0%) | 155 (7.0%) | |
Muslim | 711 (45.0%) | 1000 (45.0%) | |
Other | 63 (4.0%) | 89 (4.0%) |
Variables | Post-Vaccination Immunity, Yes (n=1580) | Post-Vaccination Immunity, No (n=2222) | p-value |
|---|---|---|---|
Diabetes | 0.001 | ||
Yes | 127 (8.0%) | 215 (9.7%) | |
No | 1453 (92.0%) | 2007 (90.3%) | |
Hypertension and other CVD | < 0.001 | ||
Yes | 380 (24.1%) | 761 (34.2%) | |
No | 1200 (75.9%) | 1461 (65.8%) | |
Sickle cell disease | 0.68 | ||
Yes | 79 (5.0%) | 111 (5.0%) | |
No | 1501 (95.0%) | 2111 (95.0%) | |
Kidney failure | 0.15 | ||
Yes | 63 (4.0%) | 89 (4.0%) | |
No | 1517 (96.0%) | 2133 (96.0%) |
Explanatory variables | Post-vaccination immunity | |
|---|---|---|
adjusted OR [95% CI] | p | |
Age | 1.56 [1.09-2.59] | 0.01 |
Residence within the sanitary cordon (yes) | 1.34 [1.14-3.01] | 0.006 |
History of hypertension and other CVD (yes) | 3.25 [1.41-4.63] | 0.000 |
History of diabetes (yes) | 2.73 [1.89-3.93] | 0.000 |
CVD | Cardiovascular Diseases |
EDTA | Ethylenediaminetetraacetic Acid |
ELISA | Enzyme-Linked Immunosorbent Assay |
IgG | Immunoglobulin G |
NLVHF | National Laboratory for Viral Hemorrhagic Fevers |
NCP | Nucleocapsid Protein |
OD | Optical Density |
SARS-CoV-2 | Severe Acute Respiratory Syndrome Coronavirus 2 |
WHO | World Health Organization |
| [1] | World Health Organization. COVID-19 Weekly Epidemiological Update. Geneva: WHO; 2020. |
| [2] | Lawal, Y. Africa's low COVID-19 mortality rate: A paradox? International Journal of Infectious Diseases. 2021, 102, 118-122. |
| [3] | Nkengasong, J. N., Mankoula, W. LOOMING THREAT: COVID-19 in Africa. Acta Scientific Microbiology. 2020, 3(6), 01-02. |
| [4] | Fontanet, A., Cauchemez, S. COVID-19 herd immunity: Where are we? Nature Reviews Immunology. 2020, 20(10), 583-584. |
| [5] | Adelakun, O. COVID-19 Vaccination in West Africa: Challenges and Prospects. Pan African Medical Journal. 2021, 38, 15. |
| [6] | Ministry of Health of Benin. COVID-19 Situation Report. Cotonou: MS; 2022. |
| [7] | Krammer, F. SARS-CoV-2 vaccines in development. Nature. 2020, 586(7830), 516-527. |
| [8] | To, K. K., Tsang, O. T., Leung, W. S., et al. Temporal profiles of viral load in posterior oropharyngeal saliva samples and serum antibody responses during infection by SARS-CoV-2: an observational cohort study. The Lancet Infectious Diseases. 2020, 20(5), 565-574. |
| [9] | Riou, C., Jasson, T. Distinct antibody responses to SARS-CoV-2 in children and adults across the COVID-19 clinical spectrum. Science Immunology. 2021, 6(57), eabd4250. |
| [10] | Ward, H., Cooke, G. Prevalence of antibody positivity to SARS-CoV-2 following the first peak of infection in England: REACT2. The Lancet. 2021, 397(10273), 477-484. |
| [11] | Pollán, M., Pérez-Gómez, B., Pastor-Barriuso, R., et al. Prevalence of SARS-CoV-2 in Spain (ENE-COVID): a nationwide, population-based seroepidemiological study. The Lancet. 2020, 396(10250), 535-544. |
| [12] | Mulenga, L. B. SARS-CoV-2 seroprevalence in Zambia: a cross-sectional study. The Lancet Global Health. 2021, 9(6), e773-e781. |
| [13] | Wiysonge, C. S. Vaccine hesitancy in Africa. The Lancet Global Health. 2022, 10(2), e154-e155. |
| [14] | Afolabi, M. O., Wariri, O. Pandemic fatigue and the new waves of COVID-19 in Africa. Pan African Medical Journal. 2021, 38, 18. |
| [15] | Euroimmun. Anti-SARS-CoV-2 ELISA (IgG) Instruction for use. Lübeck: Euroimmun AG; 2020. |
| [16] | Salyer, S. J. The first and second waves of the COVID-19 pandemic in Africa: a cross-sectional study. The Lancet Planetary Health. 2021, 5(3), e110-e120. |
| [17] | Oleribe, O. O. COVID-19 pandemic in West Africa. Pan African Medical Journal. 2020, 35, 121. |
| [18] | Ekum, A. M. COVID-19 seroprevalence in Nigeria. International Journal of Infectious Diseases. 2022, 116, S48. |
| [19] | Halatoko, W. A. Seroprevalence of SARS-CoV-2 in Togo. Lomé Médical. 2022. |
| [20] | Palacios, R. Phase 3 trial of a COVID-19 vaccine. New England Journal of Medicine. 2021, 385(1), 1-12. |
| [21] | CDC. Underlying Medical Conditions and Severe Illness Among Adults. 2021. |
| [22] | WHO Africa. Deployment of COVID-19 vaccines: guidelines for Africa. Brazzaville: WHO; 2021. |
| [23] | Ditekemena, J. D. COVID-19 vaccine acceptance in the Democratic Republic of Congo: a cross-sectional survey. Vaccines. 2021, 9(2), 153. |
| [24] | Haas, E. J. Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel. The Lancet. 2021, 397(10287), 1819-1829. |
| [25] | Bernal, J. L. Effectiveness of Covid-19 Vaccines against the B.1.617.2 (Delta) Variant. New England Journal of Medicine. 2021, 385(7), 585-594. |
| [26] | Koffi, A. Vaccination strategies in Benin: progress report. Public Health. 2022. |
| [27] | Bajema, K. L. Effectiveness of COVID-19 mRNA Vaccines Against COVID-19–Associated Hospitalization Among Immunocompromised Adults. Morbidity and Mortality Weekly Report. 2021, 70(43), 1500-1505. |
| [28] | Levin, E. G. Waning Immune Humoral Response to BNT162b2 Covid-19 Vaccine over 6 Months. New England Journal of Medicine. 2021, 385(24), e84. |
| [29] | Naaber, P. Dynamics of antibody response to BNT162b2 vaccine after six months: a longitudinal prospective study. The Lancet Regional Health - Europe. 2021, 10, 100208. |
| [30] | Hounnankan, A. Management of the COVID-19 pandemic in Benin: the sanitary cordon. Benin Médical. 2020. |
| [31] | Kpozehouen, A. Knowledge, attitudes, and practices regarding COVID-19 in Benin: A cross-sectional study. PLOS ONE. 2020, 15(11), e0242503. |
| [32] | Badoum, G. Acceptance of COVID-19 vaccination in West Africa. Vaccinated. 2022. |
| [33] | Lazarus, J. V. A global survey of potential acceptance of a COVID-19 vaccine. Nature Medicine. 2021, 27(2), 225-228. |
| [34] | Malik, A. A. Determinants of COVID-19 vaccine acceptance in the US. EClinicalMedicine. 2020, 26, 100495. |
| [35] | Paul, E. Attitudes towards vaccines and intention to vaccinate against COVID-19: Implications for public health communications. The Lancet Regional Health - Europe. 2021, 1, 100007. |
| [36] | Gouda, Z. Impact of community leaders on vaccination in Benin. African Journal of Reproductive Health. 2023, 27(5), 45-52. |
| [37] | Togun, T. Challenges in COVID-19 research in Africa. The Lancet Respiratory Medicine. 2020, 8(11), 1073-1074. |
| [38] | Crotty, S. Hybrid Immunity. Science. 2021, 372(6549), 1392-1393. |
| [39] | Nordstrom, P. Risk of SARS-CoV-2 reinfection and COVID-19 hospitalisation in individuals with natural and hybrid immunity: a retrospective, total population cohort study in Sweden. The Lancet Infectious Diseases. 2022, 22(6), 781-790. |
| [40] | Dan, J. M. Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection. Science. 2021, 371(6529), eabf4063. |
APA Style
Padonou, S. G. R., Adegbite, R., Kaucley, L., Kpossi, C., Gnanvi, M., et al. (2026). Factors Associated with Post-vaccination Immunity Against COVID-19 in Benin. World Journal of Public Health, 11(1), 11-19. https://doi.org/10.11648/j.wjph.20261101.12
ACS Style
Padonou, S. G. R.; Adegbite, R.; Kaucley, L.; Kpossi, C.; Gnanvi, M., et al. Factors Associated with Post-vaccination Immunity Against COVID-19 in Benin. World J. Public Health 2026, 11(1), 11-19. doi: 10.11648/j.wjph.20261101.12
AMA Style
Padonou SGR, Adegbite R, Kaucley L, Kpossi C, Gnanvi M, et al. Factors Associated with Post-vaccination Immunity Against COVID-19 in Benin. World J Public Health. 2026;11(1):11-19. doi: 10.11648/j.wjph.20261101.12
@article{10.11648/j.wjph.20261101.12,
author = {Setondji Geraud Romeo Padonou and Romeo Adegbite and Landry Kaucley and Clotaire Kpossi and Mariane Gnanvi and Merveille Aniambossou and Leila Djagaly and Rilwane Yessoufou and Badirou Aguemon},
title = {Factors Associated with Post-vaccination Immunity Against COVID-19 in Benin},
journal = {World Journal of Public Health},
volume = {11},
number = {1},
pages = {11-19},
doi = {10.11648/j.wjph.20261101.12},
url = {https://doi.org/10.11648/j.wjph.20261101.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.wjph.20261101.12},
abstract = {Introduction: Vaccination remains the primary strategy against COVID-19. However, data may not reflect actual population immunity. This study aims to determine the seroprevalence of post-vaccination immunity against COVID-19 in Benin and identify associated factors. Methods: A cross- sectional descriptive and analytical study was conducted from April to September 2023 in 21 hospital centers across Benin's twelve departments and included 3802. Post-vaccination immunity was defined by the presence of anti-SARS-CoV-2 Spike IgG antibodies and the absence of anti-NCP IgG antibodies, using the Euroimmun ELISA test. Data were analyzed using STATA software with multivariate logistics regression. Results: Seroprevalence of post-vaccination immunity was 41.56%. In multivariate analysis, factors associated with this immunity were age (adjusted OR=1.56; 95% CI [1.09-2.59]), residence within the former sanitary cordon (aOR=1.34; 95% CI [1.14-3.01]), history of hypertension/cardiovascular disease (aOR=3.25; 95% CI [1.41-4.63]), and history of diabetes (aOR=2.73; 95% CI [1.89-3.93]). Conclusion: Post-vaccination immunity is higher among vulnerable groups (elderly, comorbidities) and those in strategic urban zones, reflecting the prioritization of vaccination campaigns. Recommendations are proposed to target younger populations and rural areas to strengthen collective immunity.},
year = {2026}
}
TY - JOUR T1 - Factors Associated with Post-vaccination Immunity Against COVID-19 in Benin AU - Setondji Geraud Romeo Padonou AU - Romeo Adegbite AU - Landry Kaucley AU - Clotaire Kpossi AU - Mariane Gnanvi AU - Merveille Aniambossou AU - Leila Djagaly AU - Rilwane Yessoufou AU - Badirou Aguemon Y1 - 2026/01/16 PY - 2026 N1 - https://doi.org/10.11648/j.wjph.20261101.12 DO - 10.11648/j.wjph.20261101.12 T2 - World Journal of Public Health JF - World Journal of Public Health JO - World Journal of Public Health SP - 11 EP - 19 PB - Science Publishing Group SN - 2637-6059 UR - https://doi.org/10.11648/j.wjph.20261101.12 AB - Introduction: Vaccination remains the primary strategy against COVID-19. However, data may not reflect actual population immunity. This study aims to determine the seroprevalence of post-vaccination immunity against COVID-19 in Benin and identify associated factors. Methods: A cross- sectional descriptive and analytical study was conducted from April to September 2023 in 21 hospital centers across Benin's twelve departments and included 3802. Post-vaccination immunity was defined by the presence of anti-SARS-CoV-2 Spike IgG antibodies and the absence of anti-NCP IgG antibodies, using the Euroimmun ELISA test. Data were analyzed using STATA software with multivariate logistics regression. Results: Seroprevalence of post-vaccination immunity was 41.56%. In multivariate analysis, factors associated with this immunity were age (adjusted OR=1.56; 95% CI [1.09-2.59]), residence within the former sanitary cordon (aOR=1.34; 95% CI [1.14-3.01]), history of hypertension/cardiovascular disease (aOR=3.25; 95% CI [1.41-4.63]), and history of diabetes (aOR=2.73; 95% CI [1.89-3.93]). Conclusion: Post-vaccination immunity is higher among vulnerable groups (elderly, comorbidities) and those in strategic urban zones, reflecting the prioritization of vaccination campaigns. Recommendations are proposed to target younger populations and rural areas to strengthen collective immunity. VL - 11 IS - 1 ER -
Department of Public Health, University of Abomey-Calavi, Cotonou, Benin
Department of Infectious Diseases, Lambarene Medical Research Center, Lambarene, Gabon